 |
Case Report
Long-term survival in a pediatric patient with a left atrial sarcoma
1 MD, Division of Cardiovascular Surgery, Hospital Metropolitano, Quito, Ecuador
2 MD, PGY 2 Surgery Resident, P.U.C.E.-Hospital Metropolitano, Quito, Ecuador
3 MD, Division of General Surgery, Hospital IESS Quito Sur, Quito, Ecuador
4 MD, Division of Pathology, Hospital Metropolitano, Quito, Ecuador
5 MD, Division of Pediatric Oncology, Hospital Metropolitano, Quito, Ecuador
Address correspondence to:
Santiago A Endara
MD, Edif. Diagnostico 2000, Tercer piso, Av. Mariana de Jesus Oe 7/47 y Conclina, Quito,
Ecuador
Message to Corresponding Author
Article ID: 100018C04SE2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Endara SA, Davalos GA, Zavala AB, Molina GA, Mancero JO, Eguiguren JM. Long-term survival in a pediatric patient with a left atrial sarcoma. Edorium J Cardiothorac Vasc Surg 2020;7:100018C04SE2020ABSTRACT
Introduction: Primary cardiac sarcomas are rare (20% of all primary cardiac tumors) and usually lethal (mean survival range from 9.6 to 16.5 months). Undifferentiated sarcomas account for one-third of all cardiac sarcomas incorporate in their malignant mass fibrous and pleomorphic cells. Symptoms will depend on the chambers and the cardiac structures involved. Treatment is based on complete surgical excision when possible, followed by radiotherapy and chemotherapy.
Case Report: We present the case of an 11-year-old boy who was transferred to our hospital after suffering a stroke secondary to embolization from a cardiac tumor located in the left atrium. He underwent surgical resection. Pathology showed a primary cardiac tumor consistent with an undifferentiated pleomorphic sarcoma (UPS). The patient was treated with chemotherapy after the diagnosis was confirmed with immunohistochemistry. He is now 8-years off therapy and asymptomatic.
Conclusion: Primary cardiac tumors are rare. Depending on the exact location, they can present with various symptoms, such as left- or right-sided heart failure, embolic phenomena, or heart conduction abnormalities. Due to its rarity, their diagnosis is usually late; which leads to poor prognosis. High clinical awareness and prompt treatment are essential in these rare diseases.
Keywords: Cancer, Pediatric, Pleomorphic sarcoma, Sarcoma, Tumors of the heart
INTRODUCTION
First described by O’Brien and Stout in 1964, undifferentiated pleomorphic sarcoma (UPS) has become a well-known malignant soft tissue and bone tumor rarely found in other regions. Cardiac sarcoma therapy includes, if possible, complete surgical excision, followed by chemotherapy with anthracyclines, ifosfamide, or taxanes and in some cases radiotherapy. Prognosis of cardiac sarcomas is very poor, with mean survival ranging from 9.6 to 16.5 months. A less-aggressive course seems related to left atrium (LA) location, low histologic grading with scarce cellular pleomorphism and low-mitotic activity, absence of necrosis, myxoid tumor appearance, and absence of metastases at diagnosis [1],[2].
CASE REPORT
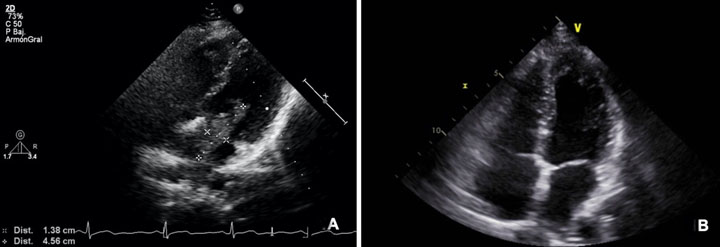
An 11-year-old boy was transferred to our hospital after presenting with one week history of gait difficulty, aphasia, involuntary eye movements, and right arm hemiparesis. He was taken to a local hospital, where symptoms were attributed to a seizure disorder; neurological focality persisted, a magnetic resonance imaging (MRI) was performed, showing reinforcement in the left temporoparietal region (compatible with ischemia). Echocardiography revealed a 4.56 × 1.38 cm tumor located in LA adherent to the posterior wall, protruding through the mitral valve toward the left ventricle causing moderate valve stenosis (Figure 1A). With these findings he was transferred to our hospital for surgical treatment, on arrival, paresis of the right upper extremity was evident, difficulty in speech and walking, but he was able to understand and follow commands. Physical examination showed cardiac arrhythmia, no murmurs. Full body computed tomography (CT) scan and chest X‑rays showed no metastatic disease.
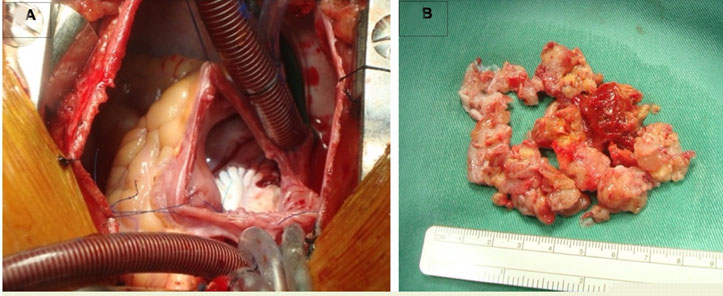
Heart surgery was performed; cardiopulmonary bypass was achieved, after aortic cross-clamping, cardiac arrest was induced by antegrade cardioplegia. After this was completed, the vena cavae were snared and a right atriotomy was done. The interatrial septum was opened just above the fossa ovalis. The 7 cm tumor was visualized and located near the pulmonary veins extending toward the interatrial septum and fossa ovalis and protruded through the mitral valve into the left ventricle. No other lesions were found during the surgical inspection (Figure 2A). The mass was removed entirely, leaving a 0.5 cm margin near the pulmonary veins. A small (1.5 cm) part of the tumor was attached to the interatrial septum. Therefore, the interauricular septum that was compromised was resected as well.
Both pulmonary veins were repaired with a continuous suture of 5-0 polypropylene; the septal defect created was restored with a synthetic cardiovascular patch sutured with 4-0 polypropylene. Both incisions on the left and right atria were closed directly by running sutures (4-0 polypropylene). The hemodynamic parameters allowed a safe weaning of the patient from cardiopulmonary bypass and sent him to the intensive care unit.
Postoperative echocardiography was performed showing no thrombus or intracardiac masses, no defects of interatrial septum or residual shunt (Figure 1B).
Pathology revealed that the tumor was composed by yellowish, fibrous areas with bleeding, irregular soft tissue fragments that weighed together 20 grams and altogether measured 10 × 8 × 2 cm (Figure 2B). Upon microscopy representative parts were processed showing an undifferentiated malignant tumor, constituted by proliferation of cells with very pleomorphic nuclei, with some large nucleoli, several atypical mitoses, and lymphocyte infiltration especially noteworthy at the edges (Figure 3A and Figure 3B).
Immunohistochemistry was positive for Vimentin (+++/+++) (Figure 3C). Cells were negative for Keratin, Actin, Desmin, CD43, CD3, CD5, S-100, EMA, PAX 5, CD30, and ALK. Based on these histomorphological and immunohistochemical findings a diagnosis of UPS was established and confirmed by pathology review studies done in the United States with a complementary immunohistochemical panel that was positive for α-1-antitrypsin, lysozyme, CD68, and MIB-1 (80%).
The patient started chemotherapy (17 cycles), alternating vincristine, cyclophosphamide, doxorubicin (VCD), ifosfamide, etoposide (IE), vincristine, and cyclophosphamide (VC). On week 11 of therapy, a complete evaluation, with body CT scan, bone scintigraphy, and electrocardiogram (EKG) showed no alterations, treatment finished on week 48 without adjuvant radiotherapy. All evaluations show that he remains stable after 8 years. He is currently 19-year-old and has no signs of local or distant recurrence. His recent EKG and echocardiography reports show no abnormalities; both his cardiac and neurologic conditions are normal.

DISCUSSION
Primary cardiac tumors constitute a rare pathologic entity with a global incidence range of 0.0017–0.019%. In children, the vast majority of primary cardiac sarcomas are benign and only 10% are malignant, meanwhile in adults 75% of primary cardiac tumors are benign, while 25% are malignant. Sarcomas are the most common [1].
Undifferentiated pleomorphic sarcoma, previously known as malignant fibrous histiocytoma, is typically found in the LA and represents less than 3% of malignant cardiac sarcomas [1]. This is a rare type of sarcoma, even more so in the pediatric age [2]. It is usually diagnosed when it is locally aggressive or has already metastasized.
Primary cardiac sarcomas, especially UPS, are extremely aggressive and locally invasive tumors, frequently making complete surgical excision unfeasible, which implies a dismal prognosis and a low survival rate [3].
Symptoms fluctuate according to location, size, and degree of invasiveness of the cardiac tumor. Systemic presentations such as fever, fatigue, and central nervous symptoms such as cerebral embolic symptoms are reported, this was the case in our patient. This is attributed to thrombus produced by hemodynamic changes rather than tumor fragments, since the tumor is usually not so friable. Moreover, patients can be completely asymptomatic, usually when the tumors are small (<3.5 cm). Undifferentiated pleomorphic sarcoma often manifests with cardiorespiratory symptoms in which dyspnea is most common. Abdominal pain, diarrhea, appetite loss, and nausea are related with hemodynamic changes of gastrointestinal circulation and growth of the malignancy [4]. The tumor manifests a broad range of histological appearances with three-types described: storiform-pleomorphic, giant cell, and inflammatory. The mean age at diagnosis is around 42 years. Often located in the LA but can involve any site, including all chambers, mitral or tricuspid valves, and pericardium.
The gold standard therapy for cardiac UPS patients without metastases is complete surgical resection of the tumor, with metastasis being the only factor identified to impact survival rate in the literature [1].
Undifferentiated pleomorphic sarcoma displays great heterogeneity in appearance and variable cellularity, with alternating areas of spindled and epithelioid cells, sometimes with abundant eosinophilic cytoplasm and intermixed giant cells. Marked pleomorphism, high mitotic activity, and foci of necrosis are commonly reported. Chondromatous and osteosarcomatous differentiation can also be detected. Immunostaining is crucial since epithelial, neural, or endothelial markers are usually negative and Vimentin is typically positive [5].
Patients usually have poor prognosis. Median survival of those diagnosed antemortem is 9–18 months [1],[6]. The survival analysis showed the outcome is not related to variables of tumor location, size, chemotherapy/radiotherapy, and surgery [6],[7], but multimodality therapy (surgery, radiation therapy, and chemotherapy) is associated with improved survival [8]. Our patient is a long-term survivor with no evidence of disease or treatment related complications.
CONCLUSION
Primary cardiac tumors are rare. Depending on the exact location, they can present various symptoms, such as left- or right-sided heart failure, embolic phenomena, or heart conduction abnormalities. Angiosarcomas are regretfully aggressive, and when they are diagnosed, they have usually already metastasized. High clinical awareness and earlier detection are needed to provide prompt treatment in order to increase survival rates in this deadly disease.
REFERENCE
1.
Sun J, Liu R, Wang W, et al. Primary cardiac malignant fibrous histiocytoma with vulvar metastases: A case report. Oncol Lett 2015;10(5):3153–6. [CrossRef]
[Pubmed]

2.
Alaggio R, Collini P, Randall RL, Barnette P, Million L, Coffin CM. Undifferentiated high-grade pleomorphic sarcomas in children: A clinicopathologic study of 10 cases and review of literature. Pediatr Dev Pathol 2010;13(3):209–17. [CrossRef]
[Pubmed]
3.
Terashima K, Aoyama K, Nihei K, et al. Malignant fibrous histiocytoma of the heart. Cancer 1983;52(10):1919–26. [CrossRef]
[Pubmed]
4.
Vallés-Torres J, Izquierdo-Villarroya MB, Vallejo-Gil JM, Casado-DomÃnguez JM, Roche Latasa AB, Auquilla-Clavijo P. Cardiac undifferentiated pleomorphic sarcoma mimicking left atrial myxoma. J Cardiothorac Vasc Anesth 2019;33(2):493–6. [CrossRef]
[Pubmed]
5.
Orlandi A, Ferlosio A, Roselli M, Chiariello L, Spagnoli LG. Cardiac sarcomas: An update. J Thorac Oncol 2010;5(9):1483–9. [CrossRef]
[Pubmed]
6.
Vaitiekiene A, Vaitiekus D, Urbonaite L, et al. Multidisciplinary approach to rare primary cardiac sarcoma: A case report and review. BMC Cancer 2019;19(1):529. [CrossRef]
[Pubmed]
7.
Wang JG. Primary cardiac tumors. In: Dumitrescu SI, Ţintoiu IC, Underwood MJ, editors. Right Heart Pathology. Cham: Springer International Publishing; 2018. p. 489–514.
8.
Randhawa JS, Budd GT, Randhawa M, et al. Primary cardiac sarcoma: 25-year cleveland clinic experience. Am J Clin Oncol 2016;39(6):593–9. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Santiago A Endara - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Gerardo A Davalos - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Aldo B Zavala - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Gabriel A Molina - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
José O Mancero - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
José M Eguiguren - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Santiago A Endara et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



